This week, is hosted by Bill Wong – he asks before joining this OTalk discussion, to please watch this TEDx talk by Dr. Douglene Jackson. https://www.ted.com/talks/douglene_jackson_putting_a_death_to_imposter_syndrome_more_than_just_an_idea)
One of the jobs of being a TEDx organizer is to unearth undiscovered and underrepresented perspectives. As I was making a comeback to organize TEDx events again in 2021, I was thinking about how to promote OT with the TEDx platform without breaking its rules. Fortunately, golf is one of my favorite occupations. One of the things I learned from professional golfers is using the rules to their advantage in certain situations. When I mastered my understanding the content diversity guidelines for TEDx organizers, that was when I thought, “Sure, I can’t have an all OT lineup for the TEDx events I organize. However, what if I make an honest effort to invite someone from OT to speak at every TEDx event I organize? Yes, that will make other allied health professions mad if they ever found out that my TEDx events favor OT. I will also have to explain to people why I can’t have an all OT lineup at my events. But, I also know I can’t please everybody.”
Once I identified my strategy in promoting OT through my TEDx events, I used the same strategy as other TEDx organizers when they consider who to send out invites. I asked myself the following questions-
1. What has already been published within the last month? (This is an important question because if an idea I am considering is already published, I may either have to stop exploring the topic or be mindful of that in the process of coaching the speaker I have invited.)
2. What underrepresented perspectives or undiscovered ideas from OT that the public should be aware of?
3. Who is/are the best OT practitioner(s) to invite on the TEDx stage to share one of the underrepresented perspectives or undiscovered ideas? Are they OK with working with tight timelines (since TEDx events typically are) and limited operating windows (since that’s the nature of the TEDx event license types I go for nowadays)?
Fortunately, I generally try to update my knowledge of OT TED and TEDx talks that have existed at least a few times a year. So, as I was planning Dr. Douglene Jackson’s talk in 2021, I thought about the following things. First, up until Dr. Jackson’s talk was published, we were at least 90% confident that there was no TED or TEDx talk by a black occupational therapy practitioner or student. Second, I believe that if I produced this talk by Dr. Jackson, it will be a lasting artifact for prospective black OT students to realize that they can have successful OT careers. Third, I believe it is important to set an example to the OT profession about what proactive advocacy looks like. I felt compelled to not repeat the same mistakes as our predecessors. Finally, justice, equity, diversity, and inclusion has been a popular topic in recent years. I believe it is important to step up and show OT can be a core community pillar in this issue.
As for the talk production, Dr. Jackson’s talk is actually one of the first talks where I took on the direct responsibility of coaching speakers. I was in imposter syndrome mode because I was trying to find my coaching style while knowing that I am not necessarily an expert in areas that my speakers will speak on. So, I fell back on what I learned during my training as an occupational therapist- being client-centered! The only times I have interjected are- a) making sure the audience can understand the material well; b) providing suggestions on how to make my speakers’ points stronger; c) when I need citations from speakers about their claims.
Since producing this talk and having it published, I showed it to 3 groups of my students. They all told me, “We never in our wildest dreams would think of watching a TEDx talk produced by one of our instructors. Moreover, this is such an unconventional way of how we advocate for our profession. You teach us something that no other OT/OTA instructor in the world can.” I also had some academics told me, “You were the brainchild for this talk? Not only organizing TEDx events is an unchartered territory for the rest of us, how can you find time to do this when you are already so busy?” I just said, “It is our duty to protect the OT profession. We not only need to share the word about our values to friends and families, we also need to learn about avenues to share it to the public. We have the necessary tools. But, we don’t use them in that context.”
Discussion Questions-
- Should OT be champions of justice, equity, diversity, and inclusion? Why or why not?
- What are your efforts to promote justice, equity, diversity, and inclusion?
- What are some strategies we can help in addressing diversity within OT?
- Please share your reflections for this talk.
- Feel free to provide constructive comments for this talk.
POST CHAT
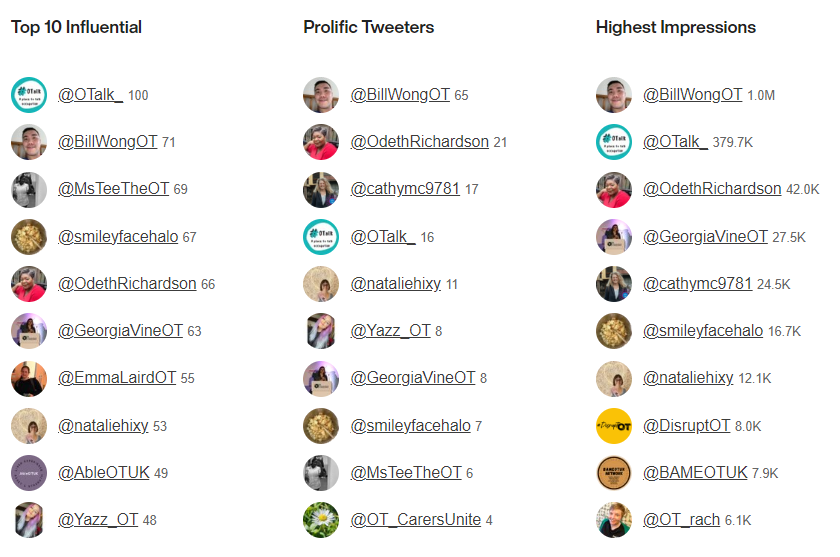
Host: Bill Wong @BillWongOT
Support on OTalk Account: Sam Pywell @smileyfacehalo
Evidence your CPD. If you joined in this chat you can download the below transcript as evidence for your CPD, but remember the HCPC are interested in what you have learnt. So why not complete one of our reflection logs to evidence your learning?
HCPC Standards for CPD.
- Maintain a continuous, up-to-date and accurate record of their CPD activities.
- Demonstrate that their CPD activities are a mixture of learning activities relevant to current or future practice.
- Seek to ensure that their CPD has contributed to the quality of their practice and service delivery.
- Seek to ensure that their CPD benefits the service user.
- Upon request, present a written profile (which must be their own work and supported by evidence) explaining how they have met the Standards for CPD.